
Management of Aortic Dissection in Marfanoid young patient with Ebstein anomaly: Rare Case Report
Abstract:
Background: Marfan syndrome is an autosomal dominant connective
tissue disorder characterized by a combination of clinical manifestations in
different organ systems. Patients with Marfan syndrome (MFS) whose lifetimes
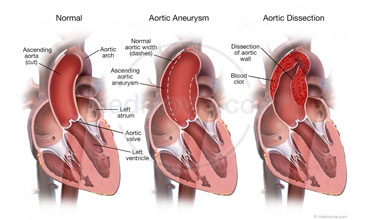
are extended may be encountered as acute abdomen cases (Aortic dissection)
apart from the obligatory reasons and emergencies arising naturally out of
their disease, as in the case reported.
Ebstein’s anomaly is a rare congenital heart disease; in which there is a
downward displacement of the tricuspid valve into the right ventricle.
Case
Report: 25-year-old Indian
male shopkeeper, 47 kg in weight and 176 cm tall was admitted in emergency
department with acute abdominal pain associated with dyspnea. Long arms and
legs, arachnodactyly, kyphoscoliosis, pectus excavatum were found to be present
in the physical examination. According to chest radiography, density increase
in the left apical field (hyperluscency) (thought to be secondary to bullous
structure), transpiring in the ascendent aorta, a rightward shift of the heart
(due to the effect of the kyphoscoliosis and pectus excavatum), and
thoracolumbar scoliosis (kyphoscoliosis) with a rightward aperture were
detected. In addition, according to the echocardiographic examination,
Ebstein’s anomaly, Aortic Dissection, Tricuspid Regurgitaion, pulmonary
hypertension, and inferior deficiency of mitral, aorta, and tricuspid valves
were present. Moreover, a right bundle block (secondary to Ebstein’s anomaly)
was observed in the electrocardiographic examination. Finally he was shifted to
cardiothoracic surgery unit for surgical repair of aortic dissection and
ebstein anomaly.
Conclusion: For cases of Marfan Syndrome (MFS), the risks of which
have been detected through a detailed cardiac examination including
echocardiography, we believe that they can be operated as emergency cases with
close anesthesia management. Mostly ascending aorta is involved with marfan
syndrome but in this case evidence of ebstein anomaly is an interesting point
towards cardiovascular surgery and learning about management and post op care.
Keywords:
Aortic dissection, marfan syndrome, ebstein anomaly.
References:
[1.]
Ades L. Guidelines for the diagnosis and management of
Marfan syndrome. Heart
Lung Circ. 2007;16:28–30.
[2.]
Attenhofer Jost CH, Connolly HM, Scott CG, Burkhart HM,
Warnes CA, Dearani JA. Outcome of cardiac surgery in patients 50 years of age
or older with Ebstein anomaly: survival and functional improvement. J Am Coll Cardiol. 2012 Jun 5. 59(23):2101-6.
[3.] Attie F, Casanova JM,
Zabal C, Buendía A, Miranda I, Rijlaarsdam M. Ebstein's anomaly. Clinical
profile in 174 patients. Arch Inst Cardiol Mex. 1999 Jan-Feb.
69(1):17-25..
[4.]
Brickner ME, Hillis LD, Lange RA. Congenital heart
disease in adults: second of two parts. N Engl J Med. 2000;342:334–342.
[5.] Brown ML, Dearani JA,
Danielson GK, Cetta F, Connolly HM, Warnes CA, et al. Effect of operation for
Ebstein anomaly on left ventricular function. Am J Cardiol. 2008 Dec 15. 102(12):1724-7.
[6.] Brown ML, Dearani JA,
Danielson GK, Cetta F, Connolly HM, Warnes CA, et al. Functional status after
operation for Ebstein anomaly: the Mayo Clinic experience. J Am Coll Cardiol. 2008 Aug 5. 52(6):460-6.
[7.] Dean JCS. Management of Marfan syndrome. Heart. 2002;88:97–103.
[8.] Groves ER. Epidural analgesia for labour in a patient
with Ebstein’s anomaly. Can J Anaesth 1995;42(1):77-79.
[9.] McGoldrick KE. Eye, ear, nose, and throat
diseases. In: Fleisher LA, editor. Anesthesia and Uncommon Disease. 5th ed. Philadelphia: Saunders Elsevier;
2006. pp. 6–7.
[10.]
Meijboom LJ, Nolle GJ, Mulder BJM. Prevention of
cardiovascular complications in the Marfan syndrome. Vas Disc Prevent. 2004;1:79–86.
[11.]
Mesrobian RB, Epps JL. Midtracheal obstruction after
Harrington rod placement in a patient with Marfan’s syndrome. Anesth Analg. 1986;65:411–413.
[12.]
Misa VS, Pan PH. Evidence based case report for analgesic
and anaesthetic management of parturient with Ebstein’s anomly and
Wolff-Parkinson- White syndrome. Int J Obstet Anesth 2007;16:77-81.
[13.]
Oh AY, Kim YH, Kim BK, et al. Unexpected tracheomalacia
in Marfan syndrome during general anesthesia for correction of scoliosis. Anesth Analg. 2002;95:331–332.
[14.] Oliver WC, Lynch JJ. Congenital heart
disease. In: Fleisher LA, editor. Anesthesia and Uncommon Disease. 5th ed. Philadelphia: Saunders Elsevier;
2006. pp. 115–118.
[15.]
Robinson PN, Godfrey M. The molecular genetics of Marfan
syndrome and related microfibrillopathies. J Med Genet. 2000;37:9–25.
[16.]
Shores J, Berger KR, Murphy EA, Pyeritz RE. Progression
of aortic dilatation and the benefit of long-term beta-adrenergic blockade in
Marfan’s syndrome. N Engl J Med. 1994;330:1335–1341.
